

Introduction
Hematopoietic cell transplantation (HCT) is a life-saving treatment option for many patients with blood disorders. Research has shown transplants occurring earlier in the disease course correlate with significantly improved outcomes (Koreth et al, JAMA, 2009). A recent study showed HLA typing with cytogenetic testing at the time of diagnosis increased the number of patients with acute myeloid leukemia (AML) receiving HCT in CR1 by 63%, resulting in a 37% increase in 2-year overall survival (Pagel et al, JCO Oncology Practice, 2020). However, many barriers still prevent patients from receiving a transplant (Majhail et al, BBMT, 2010). Applying 2018 U.S. Census estimates to the NMDP Transplant Needs Analysis (Murphy et al, BBMT, 2016) and using CIBMTR® (Center for International Blood and Marrow Transplant Research®) transplant data shows that in 2018, 49% of all AML patients in the U.S. who needed a transplant did not receive one. The goal of this research is to compare 2019 HCT referral survey data to a similar 2015 study (Meyer et al, JNCCN, 2019) and to better understand how a hematologist's/oncologist's referral patterns and perceptions of HCT may prevent patients with AML from receiving a transplant.
Methods
An online survey was conducted from September 19, 2019 - October 14, 2019 among 302 recruited, board-certified U.S. hematologists/oncologists who had seen at least 10 patients diagnosed with AML, acute lymphoblastic leukemia (ALL), or myelodysplastic syndromes (MDS) in the past year. Results focus on AML only. Pediatric-only physicians and physicians who personally perform HCT were excluded. The survey assessed the number of patients seen, referrals made, perceptions of HCT, and knowledge of National Comprehensive Cancer Network (NCCN®) AML HCT referral guidelines (NCCN®, 2020) among other topics. This survey replicated the screening criteria and questions used in the 2015 study (Meyer et al, JNCCN, 2019). T-tests and chi-square tests were used to determine changes compared to 2015 as well as differences by physician demographics.
Results
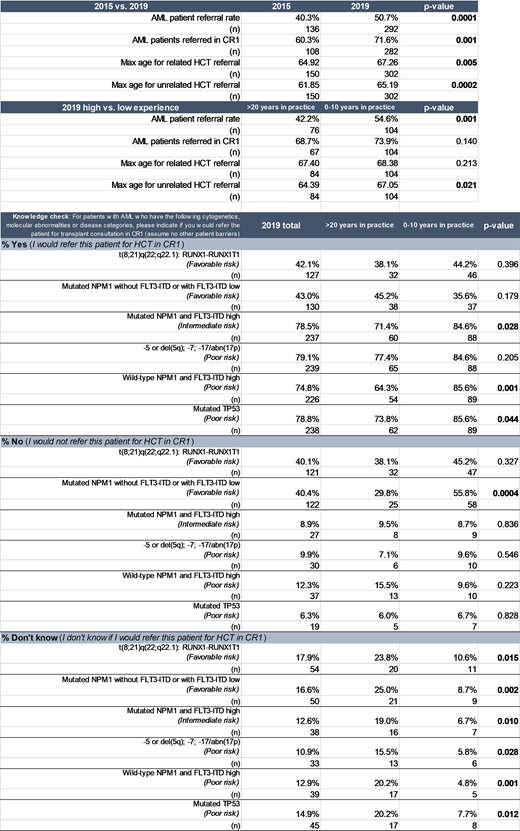
Physicians reported referring 50.7% of their patients with AML for HCT in the past 12 months in 2019, significantly higher than 40.3% as reported in 2015 (p=0.0001). Additionally, 71.6% of those patients were referred in CR1, compared to 60.3% in 2015 (p=0.001). Compared to 2015, the maximum age a physician was willing to refer any patient for transplant also increased: from 64.9 to 67.3 years for related HCT (p=0.01), and from 61.9 to 65.2 years for unrelated HCT (p=0.0002). In 2019, physicians with more years in practice (>20 years) referred a lower percentage of their AML patients for HCT in the past year compared to physicians with fewer years in practice (0-10 years) (p=0.001). In the 2019 knowledge check question based on NCCN risk stratification guidelines, 20.9%-25.5% of physicians indicated they either would not or did not know whether to refer a patient for transplant given 3 specific poor-risk cytogenetic categories, even though NCCN recommendations included referral for HCT. Physicians with more years in practice (>20 years) were significantly more likely than physicians with fewer years in practice (0-10 years) to answer that they did not know whether to refer a patient for HCT in all 6 cytogenetic/molecular marker examples shown, which included 2 favorable-risk, 1 intermediate-risk, and 3 poor-risk categories (p<0.05 for all 6 examples shown).
Discussion
While it is encouraging to see physicians referring a higher rate of patients with AML for HCT consultation, referring earlier, and referring older patients, barriers to timely HCT referral remain. Enhanced physician education regarding NCCN referral timing guidelines is recommended to ensure patients are referred for HCT consultation earlier in their disease course. Additional research is needed to understand why the number of years in practice is associated with referral rates, but an emphasis on continuing education on HCT referral guidelines could be useful, especially for physicians with more years in practice. The results of this research will be used to inform educational materials and encourage best practices, like HLA typing at diagnosis, for early transplant consultation. This will ultimately improve patient outcomes and close the HCT need gap among patients with AML.
Devine:Magenta Therapeutics: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal